

Family of Tom Fox
(from left to right: Liz, Gerry, wife Cheryl, daughter-in-law Steph, Mary, Tom, Therese John)
Our BRCA2 genetic mutation/family history is being studied at Washington University in St. Louis. UPenn’s Leonard Abramson Family Cancer Research Institute at the Abramson Cancer Center is leading the overall research, but is working with/through Washington University with our family.
Below is our family tree, representing the BRCA2 gene mutation in the Fox family. The first line represents Tom’s parents and the second line represents Tom’s siblings in age order. The children of each sibling are displayed vertically in age order below their respective parent. For ease of illustration, spouses of the children and grandchildren, as well as the great-grandchildren, are not shown.
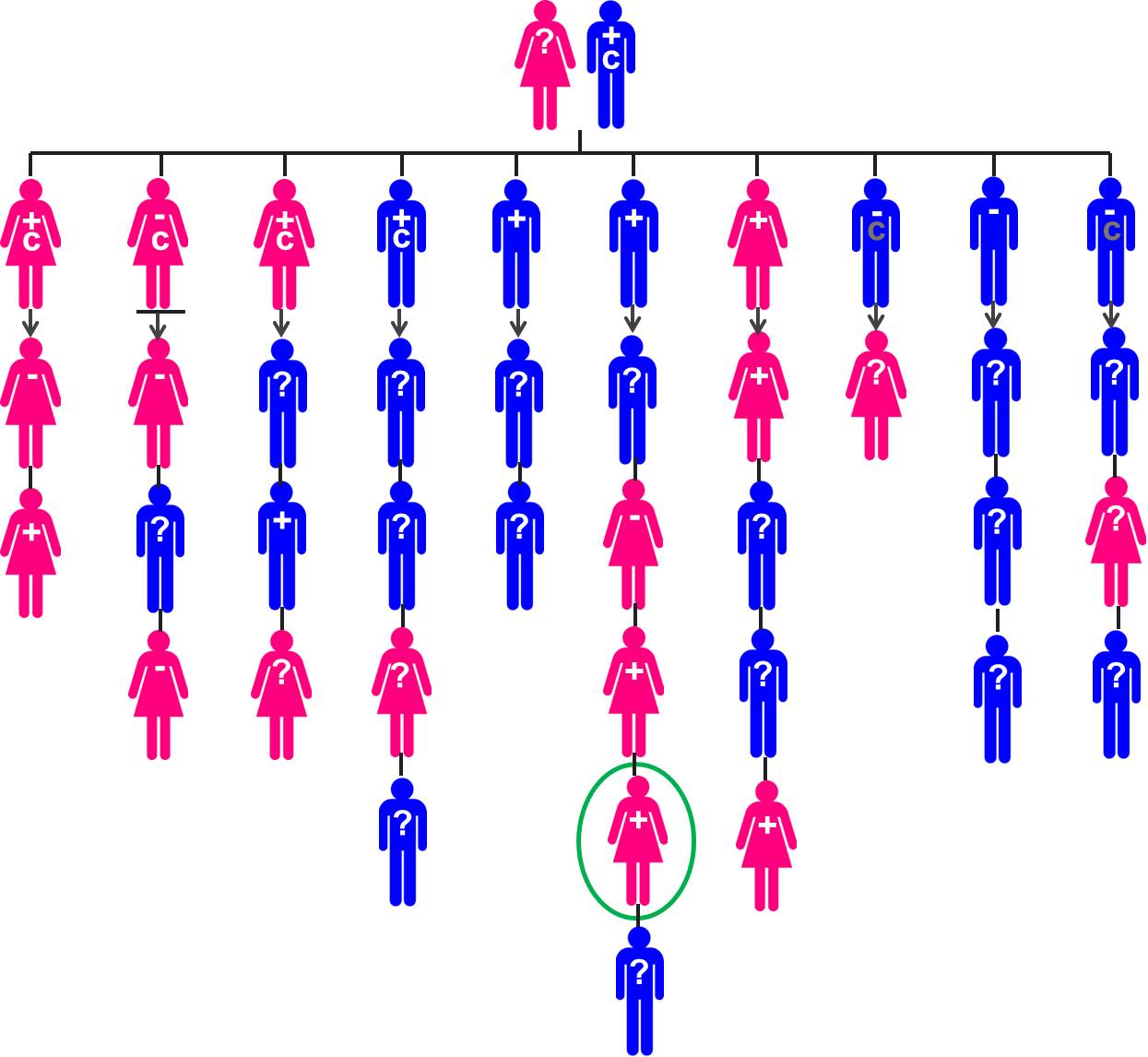
Green Circle = Therese
+ = tested positive for BRCA2
– = tested negative for BRCA2
? = not yet been tested for BRCA2
C = has had or has breast cancer
Darkened C = has had or has another type of cancer
Underlined = deceased (from cancer at age 57 after 9 years in remission)
In the Tom Fox family, Liz, Therese, and John carry the gene, Mary and Gerry do not.
Males and Breast Cancer
A number of people are surprised to hear that men can get breast cancer. Although the probability of getting breast cancer is statistically lower in males, there is still a chance particularly if they carry the BRCA1 or BRCA2 gene. Male carriers of the BRCA2 gene have a 8% risk of getting breast cancer and a 20% chance of getting prostate cancer, compared to non-carriers who have a 0.05% and 15% chance of breast and prostate cancer, respectively.
Risk Reducing Treatment for BRCA 2 Carriers
There are numerous options to manage the risk of getting breast and ovarian/prostate cancer for BRCA2 carriers. For women:
Increase Surveillance:
- Monthly breast self-exams starting at the age of 18 and clinical breast exams two times a year beginning at the age of 25
- Yearly screening with both mammography and MRI beginning at the age of 25
- Pelvic exam twice a year beginning at age 35 in patients not electing to reduce ovarian cancer risk
- Transvaginal ultrasound (an imaging technique used to create a picture of the genital tract in women by using a hand-held device inserted directly into the vagina) and testing for CA-125 levels in the blood two times a year if surgery to reduce ovarian cancer risk is not done
Risk Reducing Drug Therapy
- Drugs such as tamoxifen have been shown to reduce the risk of breast cancer in high-risk women, reducing risk by 53%
- Birth control pills may reduce the risk of ovarian cancer by up to 60%
Preventive Surgery
- Preventive mastectomy (removal of the breasts), reducing the likelihood of getting breast cancer to ~< 2%
- Preventive removal of the ovaries and fallopian tubes (oophorectomy) significantly reduces the risk of both ovarian and breast cancer by 96% and 68%, respectively
For Men
- Monthly breast self-exams and clinical breast exams two times a year beginning at age 35
- Consider a baseline mammogram at age 40
- Adhere to population screening guidelines for prostate cancer
In more recent years, many doctors have been moving away from having younger women get a mammogram and instead requiring that they get an MRI every 6 – 12 months. There is concern over the exposure to unnecessary radiation and the number of ‘false positives’ that occur resulting in unnecessary emotional and mental stress.
There is one other option that one of the doctors I met with mentioned as a treatment option of sorts, which would be more a consideration for down the line if/when I have children. A parent who has one of the BRCA mutations has a 50-50 chance of passing it on to his or her children. Women can now use reimplantation genetic diagnosis (PGD) to avoid having babies who carry the mutation. The process starts with IVF, “in which eggs are retrieved from the woman after two weeks of of hormonal stimulation, fertilized, and left to grow for five days. Then, several cells of the embryo are analyzed for BRCA mutations.” This is (clearly) controversial for obvious reasons and a very sensitive subject, but the number of women selecting to do this is on the rise. I am not stating my personal opinion on this, but as it was provided as an option for future consideration to me I wanted to include it here as well.
